

Saturday, December 15, 2018
Tuesday, December 11, 2018
Call for 2019 breech workshops
Who wants a breech workshop in their area in 2019?
Dr. David Hayes and I are thinking of blocking off a month or two in 2019 (probably August & September) to teach breech workshops around the country--and farther afield if you want us to come! Dr. Hayes is already getting inquiries from pregnant clients due in August, so he needs to decide relatively soon when to stop accepting clients.
Dr. Hayes is an obstetrician with Harvest Moon Women's Health who attends home births in Asheville, NC. He has experience attending breech in both hospital and out-of-hospital settings.
If you would like us to come teach a 2-day breech workshop near you, please let us know ASAP. We'd love to come teach breech in your area!
Your obligations:

Dr. David Hayes and I are thinking of blocking off a month or two in 2019 (probably August & September) to teach breech workshops around the country--and farther afield if you want us to come! Dr. Hayes is already getting inquiries from pregnant clients due in August, so he needs to decide relatively soon when to stop accepting clients.
Dr. Hayes is an obstetrician with Harvest Moon Women's Health who attends home births in Asheville, NC. He has experience attending breech in both hospital and out-of-hospital settings.
If you would like us to come teach a 2-day breech workshop near you, please let us know ASAP. We'd love to come teach breech in your area!
Your obligations:
- find a venue
- organize food/drinks
- advertise
- set up online ticket sales
- advertise
- teach
- provide ACNM & MEAC CEUs (we are also willing to apply for CMEs if your institution can help with that process)
Monday, December 03, 2018
Hebrides midwifery documentary by Honey Bee Pictures
I'm excited to share a guest post from filmmakers Jacob ; Honey Hesmondhalgh-Scott of Honey Bee Pictures. They are crowdfunding to support their newest documentary project.
Off the West Coast of Scotland lies some of the most remote islands in the UK, the Outer Hebrides.
With a rich cultural history, beautiful landscapes and a peaceful way of life, many thousands call these islands their home.
Living here comes with its own set of joys and challenges, but how does remote and rural midwifery impact a person’s pregnancy?
Especially if you’re unable to give birth on the island you call home.
A new feature documentary, currently in production, explores exactly this. It gives insight to the complications of pregnancy and birth in the Outer Hebrides and forms a portrait of the only midwife on the remote Isle of Barra.
Hebrides Midwifery Documentary - Trailer from Honey Bee Pictures on Vimeo.
On the Isle of Barra, Veronica, the island’s only midwife, expects 10-15 births per year, from a population of around 1,000. However, with no childbirth facilities on the island, all women leave at 38 weeks and travel to a hospital of their choosing to deliver. Meaning they could be away from home, away from family, for up to one month.
This upheaval can cause emotional, financial and physical stress. Though the NHS does provide some reimbursement, this never covers the costs in reality of moving a family away from their home.
The subsequent communication between hospitals and health boards, the crucial timing of the trip, the wellbeing of child and expectant mother, all falls to Veronica.
Previously a senior maternity co-ordinator in Lanarkshire, Veronica has been a midwife for 30 years.
Having dreamed of one day living and working in the Hebrides, 18 months ago, this became a reality and Veronica stepped back into community midwifery.
On an island with no obstetricians, gynaecologists, ultrasound equipment or labour ward, a tremendous amount of responsibility lies on veronica’s shoulders.
The Film
This independent documentary creates a striking portrait of life in the Western Isles--travelling with couples off the island across their pregnancies, flying out from the only airport in the world that lands on open beach, and learning first hand the realities of starting a family in the remote and rural Western Isles.
We hope to screen the film all over Scotland and the UK, in educational settings for universities and hospitals, international film festivals and online streaming platforms.
In other lovely news, Veronica has just been nominated for the Scotland Maternity and Midwifery Festival Achievement Award in recognition of her contribution to maternity services.
If you’re interested in supporting the film and keeping up to date with the production, we are crowdfunding to allow us to keep making the film.
If you can, please help by donating, sharing and spreading the film to your family and friends
Click here for the link and here for my Facebook page, where the film can be easily shared
To contact the filmmakers, you can get in touch through our website
www.honeybeepictures.co.uk.
Off the West Coast of Scotland lies some of the most remote islands in the UK, the Outer Hebrides.
With a rich cultural history, beautiful landscapes and a peaceful way of life, many thousands call these islands their home.
Living here comes with its own set of joys and challenges, but how does remote and rural midwifery impact a person’s pregnancy?
Especially if you’re unable to give birth on the island you call home.
A new feature documentary, currently in production, explores exactly this. It gives insight to the complications of pregnancy and birth in the Outer Hebrides and forms a portrait of the only midwife on the remote Isle of Barra.
Hebrides Midwifery Documentary - Trailer from Honey Bee Pictures on Vimeo.
On the Isle of Barra, Veronica, the island’s only midwife, expects 10-15 births per year, from a population of around 1,000. However, with no childbirth facilities on the island, all women leave at 38 weeks and travel to a hospital of their choosing to deliver. Meaning they could be away from home, away from family, for up to one month.
This upheaval can cause emotional, financial and physical stress. Though the NHS does provide some reimbursement, this never covers the costs in reality of moving a family away from their home.
The subsequent communication between hospitals and health boards, the crucial timing of the trip, the wellbeing of child and expectant mother, all falls to Veronica.
Previously a senior maternity co-ordinator in Lanarkshire, Veronica has been a midwife for 30 years.
Having dreamed of one day living and working in the Hebrides, 18 months ago, this became a reality and Veronica stepped back into community midwifery.
On an island with no obstetricians, gynaecologists, ultrasound equipment or labour ward, a tremendous amount of responsibility lies on veronica’s shoulders.
The Film
This independent documentary creates a striking portrait of life in the Western Isles--travelling with couples off the island across their pregnancies, flying out from the only airport in the world that lands on open beach, and learning first hand the realities of starting a family in the remote and rural Western Isles.
We hope to screen the film all over Scotland and the UK, in educational settings for universities and hospitals, international film festivals and online streaming platforms.
In other lovely news, Veronica has just been nominated for the Scotland Maternity and Midwifery Festival Achievement Award in recognition of her contribution to maternity services.
If you’re interested in supporting the film and keeping up to date with the production, we are crowdfunding to allow us to keep making the film.
If you can, please help by donating, sharing and spreading the film to your family and friends
Click here for the link and here for my Facebook page, where the film can be easily shared
To contact the filmmakers, you can get in touch through our website
www.honeybeepictures.co.uk.
Sunday, November 25, 2018
On your marks, get set, bake!
Over Thanksgiving weekend our kids watched several episodes of The Great British Baking Show. This inspired a round of baking today. We made a party bread stuffed with pesto, roasted butternut squash & onions, pine nuts, & sheep cheese feta.
Then we had a judging contest with Eric filling in for Paul Hollywood.
Then we had a judging contest with Eric filling in for Paul Hollywood.
Friday, November 16, 2018
My interview with Tracy Donegan of Gentlebirth
Listen to my interview about breech birth with Tracy Donegan! Tracy trained as a midwife in Ireland and currently runs GentleBirth.
The podcast is also available here on iTunes.
The podcast is also available here on iTunes.
Friday, November 09, 2018
Breech birth at home: BMC series guest blog
Dr. Stuart Fischbein and I were invited to write a guest blog about our recent article in BMC Pregnancy & Childbirth, Breech birth at home.
Here is an excerpt from my part of the blog:

Here is an excerpt from my part of the blog:
We are doing women enormous harm by taking away their bodily autonomy when their baby is breech. In theory, state and federal laws support the principle of informed consent and informed refusal, and nearly every hospital has a patient’s bill of rights that ensures consent before medical procedures. Yet we throw these legal and ethical rights away when a baby turns bottom-first.Read the rest of the blog post here.
We can do better. We owe it to the women we care for. Women should not be forced to leave the hospital in order to exercise their right to informed consent. Every woman with a breech baby deserves access to skilled providers in her own community who can support her, whether she chooses a planned cesarean section or a vaginal breech birth.
Thursday, November 08, 2018

Saturday, November 03, 2018
Asheville NC breech workshop (Dec 1-2)

A 2-day workshop on vaginal breech birth with Dr. Rixa Freeze, PhD and Dr. David Hayes, OBGYN of Harvest Moon Women's Health.
ACNM & MEAC CEUs available (7 contact hours / 0.7 CEUs)
If you are on call or cannot come in person, the event will be livestreamed and recorded.
Saturday, Dec 1:
- 9 am: Evidence on Term Breech Since the 2000 Term Breech Trial (Dr. Freeze)
- 11 am: Breech Maneuvers from 1609 to the Present (Dr. Freeze)
- 1 pm: Lunch
- 2:30-6 pm: Breech skills and hands-on simulation training (Dr. Hayes)
Sunday, Dec 2:
- 9 am: Breech Nomenclature (Dr. Freeze)
- 10:30 am: Discussion/Q&A (Dr. Hayes & Dr. Freeze)
- 12 pm: lunch
- 2-4 pm: Breech birth at home (Dr. Freeze)
Drinks & snacks provided.
Wednesday, October 31, 2018
Happy 12th birthday Zari + Halloween pictures
12 already...

Zari was a spy...

Ivy was Poison Ivy...


Dio was a bat...

Inga was the Tooth Fairy (her name, not sure how this costume has anything to do with teeth!)

Who knows what I was...but at least I finished a skirt that I had started 6+ years ago


Zari was a spy...

Ivy was Poison Ivy...


Dio was a bat...

Inga was the Tooth Fairy (her name, not sure how this costume has anything to do with teeth!)

Who knows what I was...but at least I finished a skirt that I had started 6+ years ago

Wednesday, October 24, 2018
Breech birth at home (Fischbein & Freeze 2018)
After being under consideration for a year, our article on breech birth at home was finally published! Dr. Stuart Fischbein and I analyzed the results of 60 breech and 109 cephalic pregnancies under his care. Most took place at home and some in a freestanding birth center.

The article is free to download here: https://rdcu.be/8Zv1
We chose to pay for open-access publishing so that our article would be accessible to anyone free of charge. If you'd like to help support our work, please consider donating at our GoFundMe page.
The article is free to download here: https://rdcu.be/8Zv1
We chose to pay for open-access publishing so that our article would be accessible to anyone free of charge. If you'd like to help support our work, please consider donating at our GoFundMe page.
Tuesday, September 18, 2018
Vaginal breech workshop in Decorah, IA Oct 13-14
Announcing a Breech Workshop in Decorah, IA on Oct 13-14! Please spread the word so we can re-teach breech.
I will be giving 4 lectures: evidence on term breech, breech maneuvers, breech nomenclature & risks/outcomes, and breech birth at home.
We have also two fantastic instructors for the hands-on skills portion. Cynthia Caillagh, with experience attending over 550 breech births, and Dr. David Schwartz, a family practice physician in Waukon, IA.
Livestreaming will be available if you cannot come in person or if you get called away to a birth.
ACNM & MEAC CEUs available.
Scholarships available (priority for single parents & LGBTQ birth keepers)
Click here to register

I will be giving 4 lectures: evidence on term breech, breech maneuvers, breech nomenclature & risks/outcomes, and breech birth at home.
We have also two fantastic instructors for the hands-on skills portion. Cynthia Caillagh, with experience attending over 550 breech births, and Dr. David Schwartz, a family practice physician in Waukon, IA.
Livestreaming will be available if you cannot come in person or if you get called away to a birth.
ACNM & MEAC CEUs available.
Scholarships available (priority for single parents & LGBTQ birth keepers)
Click here to register
Friday, September 07, 2018
What freediving taught me about neonatal resuscitation
This semester I am teaching a class with the theme "Exploring the Limits of the Human Body." We are currently reading Deep: Freediving, Renegade Science, and What the Ocean Tells Us About Ourselves by James Nestor. This book is a fascinating narrative that combines ocean exploration, marine biology, competitive and research freediving, and dormant human abilities that originate in our deep oceanic past (the mammalian dive reflex, magnetoreception, and echolocation).

When freedivers experience a blackout--usually near the surface at the end of their dive--they still remain responsive to sound. After pulling the unconscious freediver to the surface, the safety team will call the diver by name and tell them to breathe: "Breathe, Alexy, breathe! Breathe, Alexy, breathe!"
~~~
From my time in the home birth world, I often heard midwives talking about how they involve parents in neonatal resuscitation. A common practice is to have one of the parents speak to the baby and encourage them to breathe.
I had always categorized this practice as a nice idea. It certainly wouldn't hurt, right? In fact, I did it instinctively when Inga was born; she lost color and tone after about 30 seconds and needed mouth-to-mouth. While I was resuscitating her, I was talking to her and encouraging her to breathe.
However, I never thought that there was a scientific or physiologic reason for calling the baby by name and telling them to breathe--until I learned about freediving. Even when all of their other senses are offline, a blacked-out freediver will still respond to sound.
~~~
Calling a baby by name and telling them to breathe, especially when done by a familiar voice, isn't just fluffy woo-woo. It's part of our basic physiology.
This was a lesson in giving more respect to the instinctual or "homespun" practices that have evolved with midwifery and home birth. How many other traditions have yet-to-be-discovered science behind them?

When freedivers experience a blackout--usually near the surface at the end of their dive--they still remain responsive to sound. After pulling the unconscious freediver to the surface, the safety team will call the diver by name and tell them to breathe: "Breathe, Alexy, breathe! Breathe, Alexy, breathe!"
~~~
From my time in the home birth world, I often heard midwives talking about how they involve parents in neonatal resuscitation. A common practice is to have one of the parents speak to the baby and encourage them to breathe.
I had always categorized this practice as a nice idea. It certainly wouldn't hurt, right? In fact, I did it instinctively when Inga was born; she lost color and tone after about 30 seconds and needed mouth-to-mouth. While I was resuscitating her, I was talking to her and encouraging her to breathe.
However, I never thought that there was a scientific or physiologic reason for calling the baby by name and telling them to breathe--until I learned about freediving. Even when all of their other senses are offline, a blacked-out freediver will still respond to sound.
~~~
Calling a baby by name and telling them to breathe, especially when done by a familiar voice, isn't just fluffy woo-woo. It's part of our basic physiology.
This was a lesson in giving more respect to the instinctual or "homespun" practices that have evolved with midwifery and home birth. How many other traditions have yet-to-be-discovered science behind them?
Wednesday, July 18, 2018
Ivy's nursing party
Every time one of our children decides they are done nursing, we have a nursing party. We make or buy a cake, we nurse one last time, and then we eat the cake!
Zari was 3 1/2 and chose a strawberry & whipped cream patisserie (we were in France at the time).
Dio was also close to 3 1/2 and wanted a Lightning McQueen cake. His wasn't fancy, but he loved it.
Inga was totally done right at 2 years. Not at all interested in nursing even after I had Ivy and was producing tons of milk. I made her a chocolate cake with blackberry frosting.
Ivy has nursed the longest of everyone, several months past her 5th birthday, probably because I didn't have any other babies :) Finally she decided that she was ready for her nursing party.
So yesterday, Ivy dressed up in one of her favorite outfits, brushed her hair, and placed her barrettes in rainbow order. We walked to one of my very favorite patisserie shops, Lac. We each chose our favorite patisserie. She walked home oh-so-carefully carrying the fancy box tied up with a ribbon. We nursed one last time--the last time in my entire life! I'm going to cry! Then we ate our "nursing cakes."

I've been breastfeeding for around 11 1/2 years straight, ever since Zari was born. I'm sad and happy at ending this part of my life.
Zari was 3 1/2 and chose a strawberry & whipped cream patisserie (we were in France at the time).
Dio was also close to 3 1/2 and wanted a Lightning McQueen cake. His wasn't fancy, but he loved it.
Inga was totally done right at 2 years. Not at all interested in nursing even after I had Ivy and was producing tons of milk. I made her a chocolate cake with blackberry frosting.
Ivy has nursed the longest of everyone, several months past her 5th birthday, probably because I didn't have any other babies :) Finally she decided that she was ready for her nursing party.
So yesterday, Ivy dressed up in one of her favorite outfits, brushed her hair, and placed her barrettes in rainbow order. We walked to one of my very favorite patisserie shops, Lac. We each chose our favorite patisserie. She walked home oh-so-carefully carrying the fancy box tied up with a ribbon. We nursed one last time--the last time in my entire life! I'm going to cry! Then we ate our "nursing cakes."

I've been breastfeeding for around 11 1/2 years straight, ever since Zari was born. I'm sad and happy at ending this part of my life.
Sunday, June 24, 2018
These are my hours
These are my hours. Let them be hard. I’ll ask for what I need.

This is one of the few lines of narration in the entire documentary These Are My Hours. Filmed entirely during one woman's labor, it is the first of its kind. I'm not one to use hyperbole, so when I say that this film was revolutionary and ground-breaking and magnificent and shattering, I mean every word.
The cinematography was stunning, capturing angles and moving shots that would have been nearly impossible to choreograph--even to imagine. And let's not forget the key reason behind this film's success: Emily Graham. Her expressive face and body. Her self-monologues that range from soulful to comedic. Her deep physicality and instinctuality. Her ability to make me feel like I was there, not just watching her but there, inside her body, living the experience.
I loved that the film didn't end right at the baby's birth. Instead, we watch Emily adjust to her new body and come back to herself. We see that birth is a process with an ascent, a peak, and a descent. All three steps require navigation and integration. The descent can be just as beautiful as it has the weight of the entire experience behind it.
The filmmaker had up to 3 cameras operating simultaneously, yet I never once felt like anyone else was in the room. That was a gift and a skill on both the filmmaker's and Emily's part. The music was minimal but exceptionally powerful. And some of the scenes still take my breath away when I think about them. I won't spoil the surprise here, other than to say that you ought to watch the film. Now. It's worth every penny.
These Are My Hours is not a documentary about giving birth--it is birth. It follows Emily Graham through her labor, birth, and immediate postpartum. Or rather, we journey with her, inside her, as part of her. Besides a handful of narrative sentences and Emily's labor monologue, the documentary is almost entirely wordless. Birth is a process that transcends language and involves all of the senses, so the film's focus on the bodily experience and the near absence of language, interpretation, or commentary was fitting. I still struggle to find words adequate to describe the experience of watching These Are My Hours--a testament to the documentary's success.
As I watched this documentary, I realized: birth can speak for itself. It needs no champion or interpretation. We just have to be willing to listen.
Disclosure: I was not paid to write this, and I purchased access to the film myself.

This is one of the few lines of narration in the entire documentary These Are My Hours. Filmed entirely during one woman's labor, it is the first of its kind. I'm not one to use hyperbole, so when I say that this film was revolutionary and ground-breaking and magnificent and shattering, I mean every word.
The cinematography was stunning, capturing angles and moving shots that would have been nearly impossible to choreograph--even to imagine. And let's not forget the key reason behind this film's success: Emily Graham. Her expressive face and body. Her self-monologues that range from soulful to comedic. Her deep physicality and instinctuality. Her ability to make me feel like I was there, not just watching her but there, inside her body, living the experience.
I loved that the film didn't end right at the baby's birth. Instead, we watch Emily adjust to her new body and come back to herself. We see that birth is a process with an ascent, a peak, and a descent. All three steps require navigation and integration. The descent can be just as beautiful as it has the weight of the entire experience behind it.
The filmmaker had up to 3 cameras operating simultaneously, yet I never once felt like anyone else was in the room. That was a gift and a skill on both the filmmaker's and Emily's part. The music was minimal but exceptionally powerful. And some of the scenes still take my breath away when I think about them. I won't spoil the surprise here, other than to say that you ought to watch the film. Now. It's worth every penny.
These Are My Hours is not a documentary about giving birth--it is birth. It follows Emily Graham through her labor, birth, and immediate postpartum. Or rather, we journey with her, inside her, as part of her. Besides a handful of narrative sentences and Emily's labor monologue, the documentary is almost entirely wordless. Birth is a process that transcends language and involves all of the senses, so the film's focus on the bodily experience and the near absence of language, interpretation, or commentary was fitting. I still struggle to find words adequate to describe the experience of watching These Are My Hours--a testament to the documentary's success.
As I watched this documentary, I realized: birth can speak for itself. It needs no champion or interpretation. We just have to be willing to listen.
Disclosure: I was not paid to write this, and I purchased access to the film myself.
Friday, June 01, 2018
Aug 18-19 Breech Workshop in Auburn, WA
Come to the Aug 18-19 Breech Workshop in Auburn, WA sponsored by Dr. Rixa Freeze, Breech Without Borders, and the Washington Alliance for Responsible Midwifery (WARM).
CEUs will be available (ACNM approved; MEAC applied for).
If you can't come in person, you can livestream the conference. We will also be recording and offering the workshops online.
I am presenting four lectures on Aug 18th, mostly theoretical/informational. Aug 19th will be taught by WARM and will focus on hands-on skills and applied practice.
Online registration here.

CEUs will be available (ACNM approved; MEAC applied for).
If you can't come in person, you can livestream the conference. We will also be recording and offering the workshops online.
I am presenting four lectures on Aug 18th, mostly theoretical/informational. Aug 19th will be taught by WARM and will focus on hands-on skills and applied practice.
Online registration here.

Wednesday, May 09, 2018
Obstetric violence--where #metoo births birth
Obstetric violence is a real thing. It's a form of physical and sexual assault. It comes in many forms--from little things like clamping the cord when the mother has specifically said "no," to big things like non-consensual episiotomies or cesareans. I've seen it happen as a doula, and I've written about it in my PhD dissertation.
This recent article by Sarah Yahr Tucker knocks it out of the park: Doctors Frequently Abuse, Coerce, and Bully Women in Labor, Doulas Say.

If you want to make a difference, please donate to the "Mother May I?" documentary. If you donate today or tomorrow, a generous donor has offered a $5000 matching grant. Only 6 days left to fund the documentary!
This recent article by Sarah Yahr Tucker knocks it out of the park: Doctors Frequently Abuse, Coerce, and Bully Women in Labor, Doulas Say.
If you want to make a difference, please donate to the "Mother May I?" documentary. If you donate today or tomorrow, a generous donor has offered a $5000 matching grant. Only 6 days left to fund the documentary!
Tuesday, May 01, 2018
Announcing...Breech Without Borders
I'm excited to announce a new nonprofit initiative called Breech Without Borders (www.breechwithoutborders.org).
Breech Without Borders is an organization dedicated to disseminating knowledge about breech pregnancy and birth. It helps information cross linguistic, geographic, and knowledge borders by:

Our website is a placeholder site until we can get a professionally designed site created. We already have a few translations done in French, German, and Dutch.
If you have a skill that you would like to contribute to Breech Without Borders--illustration, graphic design, translation, accounting, grant writing, etc--please get in touch with me.
Here are a few things we need help with specifically:
1. Someone to serve as Treasurer on the Board of Directors--preferably with accounting experience and/or familiarity with the financial requirements of US nonprofits.
If you can help in this capacity but don't want to be on the Board, I'd love you bring you on as an adviser to the Treasurer. (We have one volunteer already for the position, but she isn't familiar with US nonprofits, so I'm still open to finding a person with the right background).
2. Someone with medical illustration skills. I have several projects that need a series of illustrations.
3. Translations! We can always use more volunteer translators.
I'm in the process of writing the articles of incorporation and registering the nonprofit with state & federal governments. I'm really excited to get this project started!
Breech Without Borders is an organization dedicated to disseminating knowledge about breech pregnancy and birth. It helps information cross linguistic, geographic, and knowledge borders by:
- Translating existing material about breech into multiple languages
- Supporting breech research, publication, conferences, lectures, and training workshops
- Making information about breech more accessible and understandable to both health care providers and to the public

Our website is a placeholder site until we can get a professionally designed site created. We already have a few translations done in French, German, and Dutch.
If you have a skill that you would like to contribute to Breech Without Borders--illustration, graphic design, translation, accounting, grant writing, etc--please get in touch with me.
Here are a few things we need help with specifically:
1. Someone to serve as Treasurer on the Board of Directors--preferably with accounting experience and/or familiarity with the financial requirements of US nonprofits.
If you can help in this capacity but don't want to be on the Board, I'd love you bring you on as an adviser to the Treasurer. (We have one volunteer already for the position, but she isn't familiar with US nonprofits, so I'm still open to finding a person with the right background).
2. Someone with medical illustration skills. I have several projects that need a series of illustrations.
3. Translations! We can always use more volunteer translators.
I'm in the process of writing the articles of incorporation and registering the nonprofit with state & federal governments. I'm really excited to get this project started!
Monday, April 30, 2018
Illustrations of the breech mechanisms from a 1908 French textbook
This textbook by Farabeuf and Henri V is over a century old, but the illustrations are still some of the best I've ever seen. The attention to detail, the lifelike appearance of the fetus...beautiful.
These are the complete set of illustrations from the chapter on the mechanisms of breech birth. There are other chapters on how to diagnose type of presentation by touch, interventions (maneuvers), and how to perform but full & partial breech extractions.
To reflect today's increased interest in upright breech birth, I have rotated some images to keep the maternal spine consistently upright.















These are the complete set of illustrations from the chapter on the mechanisms of breech birth. There are other chapters on how to diagnose type of presentation by touch, interventions (maneuvers), and how to perform but full & partial breech extractions.
To reflect today's increased interest in upright breech birth, I have rotated some images to keep the maternal spine consistently upright.















Friday, April 06, 2018
10 mechanisms of upright physiological breech birth
This short video shows 10 key mechanisms of a normal upright breech birth.
1. Buttocks/feet emerge sacrum-transverse
2. Body restitutes to sacrum-anterior as trunk is born
3. Legs release spontaneously
4. “Cleavage” indicates arms are not behind head
5. Baby does tummy crunches to bring down arms & flex head
6. Arms release spontaneously
7. Full perineum = head is flexed
8. Head releases spontaneously
9. Baby passed to mother
10. Cord left intact even if resuscitation is needed
When these mechanisms are present, there's no need to do anything other than catch the baby. Approximately 70% of upright breech births will occur spontaneously with no need for any hands-on maneuvers. See Louwen 2017 for more information.
The original footage is taken from a longer video of a Brazilian couple whose planned homebirth ended up at a hospital due to breech presentation. I wrote about it several months ago here.
1. Buttocks/feet emerge sacrum-transverse
2. Body restitutes to sacrum-anterior as trunk is born
3. Legs release spontaneously
4. “Cleavage” indicates arms are not behind head
5. Baby does tummy crunches to bring down arms & flex head
6. Arms release spontaneously
7. Full perineum = head is flexed
8. Head releases spontaneously
9. Baby passed to mother
10. Cord left intact even if resuscitation is needed
When these mechanisms are present, there's no need to do anything other than catch the baby. Approximately 70% of upright breech births will occur spontaneously with no need for any hands-on maneuvers. See Louwen 2017 for more information.
The original footage is taken from a longer video of a Brazilian couple whose planned homebirth ended up at a hospital due to breech presentation. I wrote about it several months ago here.
Wednesday, April 04, 2018
Need help starting a breech-related nonprofit
I have an idea for a breech-related nonprofit organization. I think it's an amazing idea, and it dovetails nicely into the work I've already been doing with breech.
Here's a brief vision of what this nonprofit would do:
1) Translate breech knowledge across languages & geographic borders. This could involve translating research articles, presentations, lectures, blog posts, birth stories, guidelines, etc. I want to do English to multiple languages and vice-versa.
2) Translate medical knowledge and research about breech into information that regular people can understand.
3) Make research and information about breech more accessible to doctors and midwives--most of whom don't have the time or interest to do all the heavy research and analysis.
I have an amazing name already picked out, but it's SUPER SECRET for the moment.
If I were to get this going, I'd need help with the following:
I want to start with French, Spanish, German, and Russian and then add as many other languages as I can find translators for.
If you're interested and/or can contribute in some way, please PM me on Facebook (preferred) or send an email. I'll add you to a Messenger conversation and we'll go from there
 |
| Illustration by Eloïse R. and used with permission |
Here's a brief vision of what this nonprofit would do:
1) Translate breech knowledge across languages & geographic borders. This could involve translating research articles, presentations, lectures, blog posts, birth stories, guidelines, etc. I want to do English to multiple languages and vice-versa.
2) Translate medical knowledge and research about breech into information that regular people can understand.
3) Make research and information about breech more accessible to doctors and midwives--most of whom don't have the time or interest to do all the heavy research and analysis.
I have an amazing name already picked out, but it's SUPER SECRET for the moment.
If I were to get this going, I'd need help with the following:
- setting up the 501(c)3 nonprofit
- website creation & hosting
- graphic design (because looks are important!)
- managing finances/accounting
- people willing to serve on the board of directors
- grant writers
- $$$ to help fund all of the above
I want to start with French, Spanish, German, and Russian and then add as many other languages as I can find translators for.
If you're interested and/or can contribute in some way, please PM me on Facebook (preferred) or send an email. I'll add you to a Messenger conversation and we'll go from there
Wednesday, March 14, 2018
Ski week at Vialattea
We got back from a week skiing in Vialattea, an inter-connected group of ski resorts in Italy & France (Sestriere, Sauze d'Oulx, Pragelato, Claviere, Cesana, Sansicario, and Montgenèvre).
We had lots of misadventures:
1) Our 2004 Opel Zafira broke down just as we got onto the freeway. The clutch was toast. We had to hobble back to Nice in 1st gear with the engine smoking. The repair would have cost far more than the car was worth, so we ended up buying a new (to us) car.
2) As Eric was packing the skis into the back of the (new) car, someone opened up the front door and stole his purse: wallet, phones, French visa, driver's license, credit cards, everything. What audacity. The thieves got away with a grand total of $30 USD, a book by Dan Chaon, and a nice leather purse that I made Eric several years ago. I'd rather pay people money NOT to steal his wallet as it's a pain to replace everything.
3) We got stuck in an icy parking lot and had to use our chains to get out. It was the only time we needed the chains, though, despite huge snowfalls right before we arrived.
4) The back of Zari's ski boot broke off while she was skiing in powder. I've never seen this happen before! She had to go down the mountain on one ski and buy new (used) boots.
Even when we weren't on the slopes, we had fun during our ski week.
Ski bloopers
We had lots of misadventures:
1) Our 2004 Opel Zafira broke down just as we got onto the freeway. The clutch was toast. We had to hobble back to Nice in 1st gear with the engine smoking. The repair would have cost far more than the car was worth, so we ended up buying a new (to us) car.
2) As Eric was packing the skis into the back of the (new) car, someone opened up the front door and stole his purse: wallet, phones, French visa, driver's license, credit cards, everything. What audacity. The thieves got away with a grand total of $30 USD, a book by Dan Chaon, and a nice leather purse that I made Eric several years ago. I'd rather pay people money NOT to steal his wallet as it's a pain to replace everything.
3) We got stuck in an icy parking lot and had to use our chains to get out. It was the only time we needed the chains, though, despite huge snowfalls right before we arrived.
4) The back of Zari's ski boot broke off while she was skiing in powder. I've never seen this happen before! She had to go down the mountain on one ski and buy new (used) boots.
Even when we weren't on the slopes, we had fun during our ski week.
Ski bloopers
Friday, March 02, 2018
Happy 7th birthday Inga!
A smile full of new teeth coming in, boundless energy and enthusiasm, solitary at times, talkative at other times--that's our Inga.

Inga's birth story, part 1
Part 2: Reflections
Part 3: Resuscitation
Part 4: Final reflections
1st birthday
2nd birthday
Inga's weaning party
3rd birthday (which I missed because I was in Seattle with Eric and Ivy...)
4th birthday

Inga's birth story, part 1
Part 2: Reflections
Part 3: Resuscitation
Part 4: Final reflections
1st birthday
2nd birthday
Inga's weaning party
3rd birthday (which I missed because I was in Seattle with Eric and Ivy...)
4th birthday
Thursday, February 15, 2018
French advice on nonfrank breech birth: apply counter-pressure to the emerging foot/feet
I'm wading through obstetrical literature of the 1980s & 1990s to discover information relating to type of breech presentation and the associated risks/outcomes.
In a 1981 article by J. Dubois, Some present aspects of the problems of breech presentation and delivery, he gives advice on attending nonfrank vaginal breech births. From p. 489:

The last part struck me, as it echoes a technique proposed by Russian obstetrician Tsovianov, the Tsovianov II. This maneuver converts a footling breech into a complete breech.
Dubois' recommendations do not mention the goal of converting leg position, but that could be a side result of counter-pressure against the feet. This technique could provide additional time for the cervix to dilate, if not already fully dilated.
In a 1981 article by J. Dubois, Some present aspects of the problems of breech presentation and delivery, he gives advice on attending nonfrank vaginal breech births. From p. 489:
#6. The nonfrank breech. We have already seen how it can pose some particular problems. If one decides to attempt a vaginal breech birth, one should take, at a minimum, 3 precautions: keep the membranes intact until full dilation; be on guard for cord presentation or cord prolapse; at the moment of expulsion, slow the emergence of the foot/feet for at least a little while by pressing one hand against the vulva.By implication, the last precaution refers specifically to breeches emerging feet-first, aka footling breech, and perhaps also to a complete breech with the foot/feet slightly in front of the buttocks. The French obstetrical nomenclature doesn't generally have a specific term for footling, just nonfrank (siège complet) and frank (siège décomplété).
The last part struck me, as it echoes a technique proposed by Russian obstetrician Tsovianov, the Tsovianov II. This maneuver converts a footling breech into a complete breech.
 |
| Antonín Doležal. Porodnické operace. 2007 |
Dubois' recommendations do not mention the goal of converting leg position, but that could be a side result of counter-pressure against the feet. This technique could provide additional time for the cervix to dilate, if not already fully dilated.
Monday, February 05, 2018
Severe acute maternal morbidity (SAMM)
Severe acute maternal morbidity (SAMM) is a maternal life-threatening event shortly before or after childbirth, often referred to as a "near miss."
Mantel et al (1998) describe a near miss as "a patient with an acute organ system dysfunction, which if not treated appropriately, could result in death." In other words, "A very ill pregnant or recently delivered woman who would have died had it not been that luck and good care was on her side."
In 2010, van Dillen et al published a study about severe acute maternal morbidity in The Netherlands. Following all pregnant women nationwide, they found that SAMM occurred 6.4 times per 1000 after elective cesarean section, compared to 3.9/1000 after planned vaginal birth. The risk of SAMM after a cesarean section persisted into the next pregnancy. The authors report: "Women with a previous CS were at increased risk for SAMM in their present pregnancy."
I created an infographic that represents those findings. Whenever a woman faces the possibility of a cesarean section, the short- and long-term risk to herself should be part of the discussion.

Mantel et al (1998) describe a near miss as "a patient with an acute organ system dysfunction, which if not treated appropriately, could result in death." In other words, "A very ill pregnant or recently delivered woman who would have died had it not been that luck and good care was on her side."
In 2010, van Dillen et al published a study about severe acute maternal morbidity in The Netherlands. Following all pregnant women nationwide, they found that SAMM occurred 6.4 times per 1000 after elective cesarean section, compared to 3.9/1000 after planned vaginal birth. The risk of SAMM after a cesarean section persisted into the next pregnancy. The authors report: "Women with a previous CS were at increased risk for SAMM in their present pregnancy."
I created an infographic that represents those findings. Whenever a woman faces the possibility of a cesarean section, the short- and long-term risk to herself should be part of the discussion.

Friday, February 02, 2018
Can we predict the likelihood of a successful vaginal breech birth?
How likely is a woman to have a cesarean when she is in labor with a breech baby? Is there any way to predict her chances of a vaginal birth based on how dilation and estimated fetal weight?
A teaching hospital in Liverpool compiled data on all singleton term and near-term breech babies born in their unit between 1988 and 1991. Nwosu et al (1993) calculated the likelihood of having an in-labor cesarean based on both estimated fetal weight and cervical dilation at admission. They explain:
Cervical dilation at admission depends on how long the mother waits to go in, so this is a tricky thing to use as a predictive measure. There is no automatic set point at which women go to hospital (or, at home, call their midwife). A woman's likelihood of a vaginal breech birth also varies widely by hospital and by provider. But this does suggest that a rapidly progressing labor is a strong positive indicator of a successful vaginal breech birth.

A teaching hospital in Liverpool compiled data on all singleton term and near-term breech babies born in their unit between 1988 and 1991. Nwosu et al (1993) calculated the likelihood of having an in-labor cesarean based on both estimated fetal weight and cervical dilation at admission. They explain:
Recently Chadha et al (1992) have shown that women admitted in labour with breech presentation at a low cervical dilatation (less than 3 cm) are more likely to be delivered by caesarean section. This is in agreement with our study. Using our results for all vaginal and emergency caesarean deliveries, we are able to tabulate the likelihood of caesarean section corresponding to various values of cervical dilatation on presentation and estimated fetal weight. These results are presented as Fig. 1 (Callygram), which could assist the clinician on the labour ward in counselling the woman, and in the choice of the best mode of delivery. It must be stressed that the tabulated (percentage) probabilities of caesarean section for given values of cervical dilatation and fetal weight are derived from our sample which has not specifically addressed the question of augmentation of labour [this unit did not induce or augment] and intrapartum external cephalic version (with or without tocolytics).As you can see, the likelihood of a successful vaginal birth increases significantly with higher cervical dilation at hospital admission. EFW also plays a role, but that difference nearly disappears at both extremes of cervical dilation.
Cervical dilation at admission depends on how long the mother waits to go in, so this is a tricky thing to use as a predictive measure. There is no automatic set point at which women go to hospital (or, at home, call their midwife). A woman's likelihood of a vaginal breech birth also varies widely by hospital and by provider. But this does suggest that a rapidly progressing labor is a strong positive indicator of a successful vaginal breech birth.

Monday, January 29, 2018
How does the 2000 Term Breech Trial compare to more recent evidence on term breech?
Recent studies do not support the findings of the 2000 Term Breech Trial, a randomized controlled trial that enrolled 2,088 women.
Two large multi-center studies in France and Belgium found no difference in perinatal/neonatal mortality between planned CS and planned vaginal birth. These studies--one prospective, one retrospective--followed a total of 10,200 women and had 174 & 175 participating hospitals.
Some national registry studies have found no significant differences between planned CS and planned vaginal breech birth.
A meta-analysis and other registry studies have found some advantage to planned CS, but the advantage is significantly less pronounced than in the Term Breech Trial.

Two large multi-center studies in France and Belgium found no difference in perinatal/neonatal mortality between planned CS and planned vaginal birth. These studies--one prospective, one retrospective--followed a total of 10,200 women and had 174 & 175 participating hospitals.
Some national registry studies have found no significant differences between planned CS and planned vaginal breech birth.
A meta-analysis and other registry studies have found some advantage to planned CS, but the advantage is significantly less pronounced than in the Term Breech Trial.

Sunday, January 28, 2018
What would happen if all Dutch women had a planned c-section for breech?
Each year around 6,490 women in the Netherlands (40%) still plan a vaginal breech birth. This number is significantly lower than it was before the 2000 Term Breech Trial, where roughly 75% planned a vaginal breech birth and around 50% overall gave birth vaginally to their breech babies (see Rietberg et al 2003).
A national registry study by Vlemmix et al (2014) calculated the anticipated neonatal benefits if these remaining 6,490 Dutch women all planned c-sections.

In several national registry studies, planned CS for breech leads to small but measurable improvements in short-term neonatal outcomes (mortality and morbidity). However, these improvements are consistently much smaller than the Term Breech Trial's findings.

This pressing question remains: at what point do the short- and long-term risks of routine cesarean begin to outweigh the short-term benefits to the baby? How many elective cesareans are justified to save 1 baby? What if women are forced into having these cesareans?
A policy of routine cesarean for breech does not allow women to decide what the acceptable risk/benefit trade-off is.

A national registry study by Vlemmix et al (2014) calculated the anticipated neonatal benefits if these remaining 6,490 Dutch women all planned c-sections.
If all women who nowadays still undergo a planned vaginal breech birth were to receive an elective cesarean, 6490 more elective cesareans would be performed. This would lead to an additional annual reduction of 10 neonatal mortalities, 116 neonates with low Apgar scores and 20 neonates with birth traumata.This calculation only considers short-term neonatal benefits--not long-term neonatal outcomes, not short- or long-term maternal outcomes. Here is another way of understanding these numbers:

In several national registry studies, planned CS for breech leads to small but measurable improvements in short-term neonatal outcomes (mortality and morbidity). However, these improvements are consistently much smaller than the Term Breech Trial's findings.

This pressing question remains: at what point do the short- and long-term risks of routine cesarean begin to outweigh the short-term benefits to the baby? How many elective cesareans are justified to save 1 baby? What if women are forced into having these cesareans?
A policy of routine cesarean for breech does not allow women to decide what the acceptable risk/benefit trade-off is.

Saturday, January 27, 2018
Friday, January 26, 2018
Risk-benefit calculus for breech presentation
Making a decision about how to birth a breech baby involves a complex risk calculus. Women have to weigh the short- and long-term benefits to themselves, their babies, and their future pregnancies. This graphic (created for me by Lauren McClain of Better Birth Graphics) shows how planned CS for breech has affected women and their babies in the Netherlands. Verhoveen et al (2005) discuss the effects of the increase in planned CS since the Term Breech Trial, and the results show a risk trade-off.
Between 2001-2005, 8,500 women in the Netherlands had a planned CS for breech. This increase in pCS saved an estimated 19 babies, but it also led to 4 direct maternal deaths, 9 additional babies dying in future pregnancies due to the uterine scar, and 140 additional life-threatening maternal complications in future pregnancies.

Alternative version of the graphic with text embedded in the image:

Between 2001-2005, 8,500 women in the Netherlands had a planned CS for breech. This increase in pCS saved an estimated 19 babies, but it also led to 4 direct maternal deaths, 9 additional babies dying in future pregnancies due to the uterine scar, and 140 additional life-threatening maternal complications in future pregnancies.

Alternative version of the graphic with text embedded in the image:

Sunday, January 21, 2018
Perinatal mortality in term breech birth
In preparation for my Jan 24th Indie Birth webinar--Is vaginal breech birth safe?--I wanted to share this series of graphics I have created. These will be explained in more detail during the presentation.
This first illustration shows neonatal and/or perinatal mortality rates from the Term Breech Trial, two large multi-center studies in France & Belgium (PREMODA and Vendittelli), a meta-analysis of several single-center studies (Krebs), and then a series of national registry studies.
These are all studies of term breech births of singleton fetuses alive at the beginning of labor with congenital anomalies excluded (exception: the TBT also included antepartum stillbirths).
On the right of the graphic is the type of mortality studied:

For Vlemmix, Vistad, Hartnack-Tharin, and Vistad, I included only the data from the later time periods (usually post-TBT).
The next slide shows the same dataset, adding in planned cephalic births (vaginal & cesarean) analyzed in two of the registry studies.
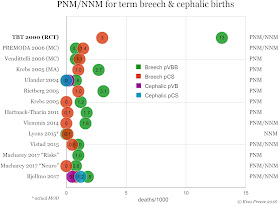
The last slide shows the relative samples sizes of the various studies. On the right side, you can see the sample sizes of the pVBB and pCS groups.

This first illustration shows neonatal and/or perinatal mortality rates from the Term Breech Trial, two large multi-center studies in France & Belgium (PREMODA and Vendittelli), a meta-analysis of several single-center studies (Krebs), and then a series of national registry studies.
These are all studies of term breech births of singleton fetuses alive at the beginning of labor with congenital anomalies excluded (exception: the TBT also included antepartum stillbirths).
On the right of the graphic is the type of mortality studied:
- PNM/NNM: intrapartum deaths + neonatal deaths up to 28 days
- PNM: intrapartum deaths + neonatal deaths up to 7 days
- NNM: infant deaths through 28 days; intrapartum stillbirths excluded

For Vlemmix, Vistad, Hartnack-Tharin, and Vistad, I included only the data from the later time periods (usually post-TBT).
The next slide shows the same dataset, adding in planned cephalic births (vaginal & cesarean) analyzed in two of the registry studies.

The last slide shows the relative samples sizes of the various studies. On the right side, you can see the sample sizes of the pVBB and pCS groups.
